Ketamine has been called the greatest breakthrough in depression research in 60 years. That is not hyperbole. It is the assessment of researchers at Yale, Harvard, and NIMH who have spent decades watching conventional antidepressants fail a third of the people who take them.
What makes ketamine genuinely remarkable isn't just that it works where SSRIs don't. It's that it works through a completely different mechanism, one that appears to physically rebuild the synaptic architecture that chronic stress and depression destroy. And it does it in hours rather than weeks.
This article covers what the science actually shows about how ketamine affects the brain: the NMDA receptor mechanism, the downstream cascade that drives neuroplasticity, the 2026 imaging study that provided the first direct human evidence of synaptic repair, and the genuinely unresolved debate between S-ketamine and R-ketamine that the field is still actively working through.
Why Conventional Antidepressants Fail, and Why Ketamine Is Different
To understand why ketamine is such a significant departure, you need to understand what it's departing from.
Traditional antidepressants, SSRIs, SNRIs, MAOIs, all work on the monoamine system. They increase serotonin, norepinephrine, or dopamine by preventing reuptake or breakdown. This approach has been the dominant framework for depression treatment since the 1950s. Despite over 60 years of antidepressant development, mood disorders remain among the most disabling medical conditions in the world. The NIMH STAR-D study indicated that only approximately one-third of depressed patients remitted on their initial antidepressant. Modest incremental benefits were seen with subsequent treatments, approximately one-third of patients remained unremitted after four treatments, and the one-year relapse rate among patients with treatment-resistant symptoms was approximately 75%.
The monoamine model also has a fundamental practical problem: it takes 4 to 12 weeks to produce clinical effects. For someone in acute crisis, that timeline is not just inconvenient: it's dangerous.
The rising prevalence of depression, with its associated suicide risk, demands effective fast-acting treatments. Ketamine has emerged as promising, demonstrating rapid antidepressant effects. While early studies show swift mood improvements, its precise mechanisms remain under investigation.
What is clear is that ketamine operates on a completely different neurotransmitter system: glutamate, not serotonin. And it produces effects in hours rather than weeks. Understanding why requires going deep into the biology.
The NMDA Receptor: What It Is and Why It Matters
N-methyl-D-aspartate receptors, commonly called NMDA receptors, are ionotropic glutamate receptors that play a central role in synaptic plasticity, learning, memory, and mood regulation. They are gated ion channels that require both glutamate binding and membrane depolarisation to open. This coincidence-detection mechanism makes them critical for the strengthening and weakening of synaptic connections.
NMDA receptors manage synaptic plasticity, keeping synapses pliable and able to retain information. Blocking NMDA receptors activates AMPA receptors to release other molecules that help brain cells communicate with each other along new pathways. This process is known as synaptogenesis and likely affects mood, thought patterns, and cognition including memory.
In depression, chronic stress produces a specific and well-documented pattern of synaptic damage. Activation of extrasynaptic NMDA receptors by extracellular glutamate contributes to excitotoxicity and synaptic atrophy, processes closely associated with depression and other neuropsychiatric disorders. This understanding has led to the hypothesis that inhibiting NMDA receptors could promote synaptic regeneration and mitigate the adverse effects of depression and stress.
The prefrontal cortex and hippocampus, the brain regions most critical for mood regulation, memory, and executive function, show measurable synaptic loss and neuronal atrophy in depressed individuals. This is not a metaphorical description of feeling bad. It is structural damage that can be measured on neuroimaging. Ketamine appears to reverse it.
How Ketamine Works: The Cascade
Ketamine's mechanism is more complex than simple NMDA receptor blockade. Understanding the full cascade explains both why it works so rapidly and why the effects can persist well beyond the drug's presence in the system.
Step 1: NMDA receptor blockade on GABAergic interneurons
According to the disinhibition model, ketamine predominantly acts on inhibitory interneurons, curtailing their tonic NMDA receptor dependent activity and in turn augmenting excitability of glutamatergic neurons as well as ensuing glutamate release.
In simpler terms: GABA is the brain's primary inhibitory neurotransmitter. Ketamine blocks NMDA receptors on the interneurons that release GABA, reducing inhibition on excitatory glutamate neurons. This produces what researchers call a glutamate surge.
Step 2: AMPA receptor activation and the mTOR pathway
Ketamine primarily works by antagonizing NMDA receptors, reducing GABAergic inhibition, and increasing glutamate release. This enhanced glutamate activates AMPA receptors, triggering crucial downstream cascades, including BDNF-TrkB and mTOR pathways, promoting synaptic proliferation and regeneration.
The mTOR pathway, mechanistic target of rapamycin, is a master regulator of cell growth, protein synthesis, and survival. mTOR is triggered by both the activation of AMPA receptors and the antagonism of NMDA receptors from ketamine binding. This protein kinase has many upstream and downstream effectors and responds to various physiological cues such as amino acids, stress, growth factors, and metabolism.
Step 3: BDNF release and synaptic repair
Brain-Derived Neurotrophic Factor, BDNF, is the molecule most directly responsible for ketamine's structural effects on the brain. BDNF is critical for neuroplasticity, synaptic transmission, and neuronal survival. Its expression is significantly reduced in brain areas such as the prefrontal cortex and hippocampus in patients with depression. Ketamine and its S-enantiomer exert both rapid and sustained antidepressant effects through activation of glutamate-related pathways, with neurotrophic effects involving BDNF.
Ketamine-mediated NMDA receptor blockade ceases tonic eEF2 kinase activity, resulting in a gradual loss of eEF2 phosphorylation and de-suppression of BDNF translation, ultimately triggering TrkB receptor signaling. TrkB signaling and subsequent rapid homeostatic synaptic plasticity is required to elicit not only rapid effects of ketamine but also its sustained effects.
The sustained effects are the most clinically significant part of this. A single ketamine infusion can produce antidepressant effects that outlast the drug's presence in the system by days or weeks, because the structural changes it initiates through BDNF-TrkB-mTOR signalling persist after the molecule has cleared.
The 2026 Imaging Study: First Direct Human Evidence of Synaptic Repair
The most significant recent development in ketamine neuroscience is a 2026 study published in Molecular Psychiatry that provided something the field had never had before: direct visualisation of synaptic changes in living human brains during ketamine treatment.
Researchers used a novel PET tracer called [11C]K-2 to visualise changes in AMPA receptors in the living human brain as participants received treatment. Led by Professor Takuya Takahashi at Yokohama City University, the research team combined data from three registered clinical trials including 34 people with treatment-resistant depression and 49 healthy controls. The results revealed that people with treatment-resistant depression had widespread abnormalities in AMPA receptor density compared with healthy participants.
Ketamine did not produce uniform changes across the brain. Improvements in depressive symptoms were linked to dynamic, region-specific adjustments. Some cortical areas showed increased receptor density, while reductions appeared in regions associated with reward processing, especially the habenula. These region-specific shifts correlated closely with improvements in participants' depressive symptoms.
The clinical implication is significant. Beyond explaining how ketamine works, the findings suggest that AMPA receptor PET imaging may one day serve as a biomarker, a measurable indicator that could help clinicians predict which individuals are most likely to respond to ketamine treatment.
This study confirmed what animal models had long suggested and what clinical outcomes had implied: ketamine is not merely suppressing symptoms but actively rebuilding the neural infrastructure that depression damages.
Does Ketamine Cause Neuron Regrowth?
This question requires precision because it's frequently overstated in wellness content.
What the evidence clearly supports: ketamine promotes synaptogenesis, the formation of new synaptic connections between existing neurons. It increases dendritic spine density in the prefrontal cortex. It reverses the synaptic atrophy caused by chronic stress. It upregulates BDNF which supports neuronal survival and plasticity. It activates mTOR which drives protein synthesis necessary for structural changes.
What is less established: whether ketamine produces true neurogenesis, the birth of entirely new neurons in adult brain tissue, in humans. The animal data on hippocampal neurogenesis is promising but has not been definitively confirmed in human clinical studies.
The more accurate framing, and the one supported by the 2026 imaging data, is that ketamine restores synaptic connectivity that stress and depression have degraded. That is not a minor distinction. Rebuilding damaged neural architecture is a genuinely significant therapeutic outcome regardless of whether new neurons are involved.
S-Ketamine vs R-Ketamine: The Debate the Field Is Still Having
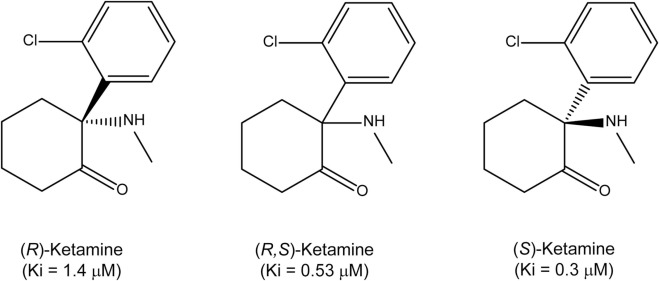
Racemic ketamine, the form used in IV infusions and most clinical settings, contains equal parts of two mirror-image molecules: S-ketamine (esketamine) and R-ketamine (arketamine). They share the same chemical formula but are oriented differently in three-dimensional space, and that difference produces meaningfully distinct pharmacological profiles.
S-Ketamine (Esketamine)
Esketamine has been found to be more potent, offering three times stronger analgesic effects and 1.5 times greater anesthetic efficacy than arketamine. It provides smoother anesthesia with fewer side effects and is widely used in clinical settings due to its neuroprotective, bronchodilatory, and antiepileptic properties. Approved by the FDA and EMA in 2019, esketamine is currently used alongside SSRIs or SNRIs for treatment-resistant depression.
The decision was made to develop the S-enantiomer because esketamine is about 4 to 5 times more potent at the NMDA receptor than the R-enantiomer. S-ketamine is available as Spravato, an intranasal spray administered at certified clinics with mandatory two-hour monitoring after each dose.
The practical advantage of esketamine is accessibility and insurance coverage. The mandatory clinic-based administration also provides safety oversight that unmonitored racemic ketamine does not.
R-Ketamine (Arketamine)
R-ketamine presents a genuinely interesting scientific puzzle. It demonstrates a milder NMDA blockade but may engage other targets including the AMPA receptor. Some studies suggest this may contribute to sustained antidepressant benefits, although the onset is slower. While S-ketamine delivers quick symptom relief, R-ketamine may play a subtler, enduring role in stabilising mood pathways.
Researchers at Translational Psychiatry confirmed that R-ketamine generates stronger antidepressant effects while sustaining its duration for a longer period than S-ketamine and produces lower psychotomimetic side effects. However, in later studies, it failed to show antidepressant effectiveness in a controlled Phase 2a clinical trial.
That last point is the crux of the R-ketamine story: compelling preclinical data that hasn't translated cleanly into controlled human trials. Early research suggested R-ketamine might offer longer-lasting effects with fewer side effects, but a controlled clinical trial found it wasn't more effective than placebo for depression. It is not currently available outside clinical trials.
Racemic Ketamine
The irony of the S vs R debate is that the racemic mixture, containing both, may outperform either enantiomer alone in real-world clinical settings. Comparative analyses suggest racemic ketamine may show higher response rates than esketamine in some meta-analyses. However, different delivery methods, IV versus nasal spray, make direct comparisons complicated.
Legitimate uncertainty remains regarding the comparative efficacy of the two drugs. An ongoing well-powered comparative effectiveness study should provide a more definitive answer, though study results will not be available until 2028 at the earliest. In the meantime there is evidence that both ketamine and esketamine can be helpful in managing treatment-resistant depression.
The honest summary: S-ketamine is FDA-approved, more potent at NMDA receptors, faster-acting, and the only form with regulated clinical infrastructure. R-ketamine shows promise in preclinical work but has not yet demonstrated superiority in controlled human trials. Racemic ketamine remains the most widely used form and may have clinical advantages that aren't fully explained by NMDA potency alone.
What Ketamine Is Not
Intellectual honesty requires acknowledging what the evidence doesn't support alongside what it does.
Ketamine is not a cure for depression. The antidepressant effects, while rapid, are time-limited without repeated dosing or integration with psychotherapy. The question of how to sustain the neuroplastic window ketamine opens, and translate it into durable psychological change, is one the field is actively working on.
Ketamine carries real risks. Common side effects include sedation in 48 to 61% of people, dissociation, and blood pressure elevation. These safety concerns are why mandatory two-hour monitoring at certified facilities is required after each dose. Repeated unsupervised use carries dependency risk and bladder toxicity at high recreational doses.
The long-term cognitive safety data is reassuring but not complete. Overall there were no cognitive differences between ketamine and control in 21 independent comparisons, except for one that favoured ketamine in delayed memory 24 hours post-dose. This is a positive signal but long-term neuropsychological outcomes with repeated therapeutic dosing require continued study.
The Integration Question
The most important insight from recent ketamine research may not be about the molecule itself but about what happens after. The brain's increased flexibility following ketamine treatment creates an opportunity to establish healthier thought patterns, emotional responses, and behavioural routines. Without integration support, those opportunities may not translate into durable change.
The neuroplastic window that ketamine opens, the period of enhanced synaptic flexibility and BDNF elevation following treatment, is genuinely valuable. But neuroplasticity is directional. A brain made more plastic is not automatically a brain made healthier. The inputs that fill that window matter enormously.
This is why the most effective ketamine protocols combine the pharmacological intervention with psychotherapy, breathwork, somatic processing, and lifestyle practices that give the enhanced plasticity somewhere constructive to go. The molecule creates the conditions for change. The integration work determines what that change becomes.
If you're exploring how to build an integration protocol around a ketamine treatment experience, a personalised guidance session can help you design a structure that makes the most of the neuroplastic window.
Sources
Molecular Psychiatry 2026. First direct human evidence of AMPA receptor changes during ketamine treatment. nushama.com
Frontiers in Neuroscience 2023. Antidepressant mechanisms of ketamine, NMDA antagonism and neuroplasticity review. frontiersin.org
MDPI International Journal of Molecular Sciences 2024. Beyond NMDA Receptors: multifaceted mechanisms of ketamine in depression. mdpi.com/1422-0067/25/24/13658
PNAS 2023. Ketamine and the neurobiology of depression: toward next-generation antidepressants. pnas.org
MDPI Brain Sciences 2025. Ketamine and esketamine comparative review with neuroplasticity focus. mdpi.com/2813-1851/4/3/20
PMC 2024. Variations in BDNF and their role in ketamine and esketamine antidepressant mechanisms. mdpi.com/1422-0067/25/23/13098
Journal of Clinical Psychiatry 2025. Ketamine and esketamine: is there a meaningful clinical difference? psychiatrist.com
Frontiers in Pharmacology 2025. Comparative safety and tolerability of ketamine and esketamine meta-analysis. frontiersin.org
Medical Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice. Ketamine and esketamine are controlled substances that should only be used under qualified medical supervision. If you are experiencing depression or suicidal ideation please contact a healthcare professional or crisis service immediately.